





 :.
:.


Sarah L. Melendez, MD; Mark A. Silverberg, MD Contributor Information

Tube thoracostomy is the insertion of a tube (chest tube) into the pleural cavity to drain air, blood, bile, pus, or other fluids. Whether the accumulation is the result of rapid traumatic filling or insidious malignant seepage, placement of a chest tube allows for continuous, large volume drainage until the underlying pathology can be more formally addressed. The list of specific treatable etiologies is extensive, but without intervention, patients are at great risk for major morbidity or mortality.

ndications for chest tube placement (thoracostomy) include the following:
- Pleural effusion (shown)
- Spontaneous or traumatic pneumothorax
- Tension pneumothorax (should be treated first with needle decompression and then with tube thoracostomy)
- Empyema
- Hemothorax
- Chylothorax

Standard instrumentation for tube thoracostomy is shown. To perform a chest tube placement, the following equipment is needed: sterile gloves, preparatory solution (chlorhexidine and/or Betadine), sterile drapes, surgical marker, two 10- to 20-mL syringes, a 25-gauge 5/8" needle, a 23-gauge 1.5” needle or 27-gauge 1.5” needle (for instilling local anesthesia), no. 10 blade on a handle, Vaseline gauze, ten 4×4 inch gauze squares, sterile adhesive tape (4" wide), 0 or 1-0 silk or nylon suture, large and small needle drivers, large and medium Kelly clamps, large curved Mayo scissors, large straight suture scissors, lidocaine, and a drainage device (with suction source and tubing).

Standard instrumentation for tube thoracostomy is shown. To perform a chest tube placement, the following equipment is needed: sterile gloves, preparatory solution (chlorhexidine and/or Betadine), sterile drapes, surgical marker, two 10- to 20-mL syringes, a 25-gauge 5/8" needle, a 23-gauge 1.5” needle or 27-gauge 1.5” needle (for instilling local anesthesia), no. 10 blade on a handle, Vaseline gauze, ten 4×4 inch gauze squares, sterile adhesive tape (4" wide), 0 or 1-0 silk or nylon suture, large and small needle drivers, large and medium Kelly clamps, large curved Mayo scissors, large straight suture scissors, lidocaine, and a drainage device (with suction source and tubing).

To begin the procedure, place the patient in a supine position or at a 45-degree angle, to reduce the risk of diaphragm elevation and improper chest tube placement. Abduct and externally rotate the arm on the patient’s affected side, so that the patient’s palm lies behind his or her head. A chest tube is typically inserted in the triangle of safety, a region delineated by the anterior border of latissimus dorsi, the lateral border of pectoralis major, and a horizontal line lateral at the level of the nipple, or about the 5th intercostal space. The tube insertion area is between the midaxillary and anterior axillary lines at the level of the nipple. Prepare and mark the skin (shown) to demarcate the relevant anatomy

nject a systemic analgesic (shown), unless contraindicated. Using the 25-gauge needle, inject 5 mL of local anesthetic solution into the skin that will overlie the initial incision. Using the 23-gauge or, preferably, 27-gauge needle, infiltrate approximately 5 mL of the anesthetic solution to a wide region of subcutaneous tissue that is superior to the targeted site of initial incision. Redirect the needle along the expected course of the chest tube. Inject approximately 10 mL of anesthetic solution into the periosteum (if bone is encountered), intercostal muscle, and pleura. Look for aspiration of air, blood, or pus into the syringe, to verify that the needle entered the pleural cavity.

Tube thoracostomy is the insertion of a tube (chest tube) into the pleural cavity to drain air, blood, bile, pus, or other fluids. Whether the accumulation is the result of rapid traumatic filling or insidious malignant seepage, placement of a chest tube allows for continuous, large volume drainage until the underlying pathology can be more formally addressed. The list of specific treatable etiologies is extensive, but without intervention, patients are at great risk for major morbidity or mortality.

ndications for chest tube placement (thoracostomy) include the following:
- Pleural effusion (shown)
- Spontaneous or traumatic pneumothorax
- Tension pneumothorax (should be treated first with needle decompression and then with tube thoracostomy)
- Empyema
- Hemothorax
- Chylothorax

Standard instrumentation for tube thoracostomy is shown. To perform a chest tube placement, the following equipment is needed: sterile gloves, preparatory solution (chlorhexidine and/or Betadine), sterile drapes, surgical marker, two 10- to 20-mL syringes, a 25-gauge 5/8" needle, a 23-gauge 1.5” needle or 27-gauge 1.5” needle (for instilling local anesthesia), no. 10 blade on a handle, Vaseline gauze, ten 4×4 inch gauze squares, sterile adhesive tape (4" wide), 0 or 1-0 silk or nylon suture, large and small needle drivers, large and medium Kelly clamps, large curved Mayo scissors, large straight suture scissors, lidocaine, and a drainage device (with suction source and tubing).
Standard instrumentation for tube thoracostomy is shown. To perform a chest tube placement, the following equipment is needed: sterile gloves, preparatory solution (chlorhexidine and/or Betadine), sterile drapes, surgical marker, two 10- to 20-mL syringes, a 25-gauge 5/8" needle, a 23-gauge 1.5” needle or 27-gauge 1.5” needle (for instilling local anesthesia), no. 10 blade on a handle, Vaseline gauze, ten 4×4 inch gauze squares, sterile adhesive tape (4" wide), 0 or 1-0 silk or nylon suture, large and small needle drivers, large and medium Kelly clamps, large curved Mayo scissors, large straight suture scissors, lidocaine, and a drainage device (with suction source and tubing).

To begin the procedure, place the patient in a supine position or at a 45-degree angle, to reduce the risk of diaphragm elevation and improper chest tube placement. Abduct and externally rotate the arm on the patient’s affected side, so that the patient’s palm lies behind his or her head. A chest tube is typically inserted in the triangle of safety, a region delineated by the anterior border of latissimus dorsi, the lateral border of pectoralis major, and a horizontal line lateral at the level of the nipple, or about the 5th intercostal space. The tube insertion area is between the midaxillary and anterior axillary lines at the level of the nipple. Prepare and mark the skin (shown) to demarcate the relevant anatomy

nject a systemic analgesic (shown), unless contraindicated. Using the 25-gauge needle, inject 5 mL of local anesthetic solution into the skin that will overlie the initial incision. Using the 23-gauge or, preferably, 27-gauge needle, infiltrate approximately 5 mL of the anesthetic solution to a wide region of subcutaneous tissue that is superior to the targeted site of initial incision. Redirect the needle along the expected course of the chest tube. Inject approximately 10 mL of anesthetic solution into the periosteum (if bone is encountered), intercostal muscle, and pleura. Look for aspiration of air, blood, or pus into the syringe, to verify that the needle entered the pleural cavity.

With the no. 10 blade, make a 4-cm horizontal skin incision (shown) above the rib that is below the desired intercostal level of entry.

Use a Kelly clamp to bluntly dissect through subcutaneous tissue and fascia (shown), creating a tract by intermittently advancing the closed instrument and opening it.

Use an index finger to palpate the tract (shown) and tunnel upward over the rib that is above the skin incision. Inject additional local anesthetic into the intercostal muscles and pleura.

Using the closed Kelly clamp, apply some force and a twisting motion to pass through the intercostal muscles and parietal pleura and enter into the pleural space (shown). Be careful to perform this motion with a controlled approach, to prevent the clamp from entering too far into the chest and potentially injuring the lung or diaphragm. Listen and feel for a pop (resulting from a rush of air or fluid) to confirm the entry of the Kelly clamp into the pleural space.

Within the pleural space, open the Kelly clamp and then withdraw it so that its jaws enlarge the dissected tract through all layers of the chest wall (shown). This will make it easier to insert the chest tube. When opening and withdrawing the Kelly clamp, the orientation of the clamp should be parallel (as opposed to perpendicular) to the rib space, in order to minimize morbidity associated with damage to the neuromuscular bundle.

Use the index finger to palpate the tract and feel for adhesions (shown). Rotate the finger by 360 degrees, to confirm the tract and try to loosen and break easily disrupted adhesions. Do not try to lyse significant, organized adhesions manually, as doing so may cause significant bleeding. Determine the distance between the incision and the apex of the lung, in order to know how far to advance the chest tube.

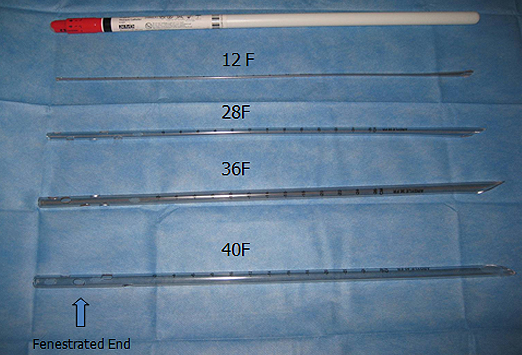
Clamp the fenestrated proximal end of the chest tube with a Kelly clamp (shown) and introduce it through the tract. Next, clamp the distal end of the chest tube until it can be connected to a drainage system, in order to prevent blood from pouring out of the tube onto the floor.

Hold the chest tube in one hand and direct it through the incision (shown), releasing the Kelly clamp proximally and pushing in posteriorly and superiorly using a circular motion.

Use the index finger of the other hand to help guide the chest tube posteriorly and superiorly (shown), using circular motion and making sure all holes are within the thoracic cavity

Make certain that the final hole is inside the thoracic cavity. This hole crosses the white line on the tube (shown) and aids in detecting it on x-rays.

Connect the chest tube’s distal end to a drainage device (shown). To make it easier to connect to the drainage device, some practitioners cut the distal end of the tube. Once the chest tube and drainage device are connected, release the cross clamp that is on the chest tube. To confirm proper intrathoracic placement, look for a respiration-related swing in the fluid level of the drainage device and for respiration-related condensation levels in the tube.

Suture the tube securely to the patient’s chest with 1-0 silk or nylon sutures (shown), using a curved or straight needle.

To secure sutures, use 2 distinct through-and-through, simple, interrupted stitches on each side of the chest tube (shown). Ensure that there are no possible areas for air to leak. Each stitch should be tied tightly to the skin, then wrapped tightly around the chest tube several times to cause slight indentation, and then tied again without breaking suture. Some physicians favor locking sutures to secure a large-bore thoracostomy tube.

Place Xeroform gauze (shown) over the skin incision. Fold the gauze on itself, wrap it around the thoracostomy tube, and then push it down to the skin insertion site to create an additional barrier

Use the index finger of the other hand to help guide the chest tube posteriorly and superiorly (shown), using circular motion and making sure all holes are within the thoracic cavity

Make certain that the final hole is inside the thoracic cavity. This hole crosses the white line on the tube (shown) and aids in detecting it on x-rays.

Connect the chest tube’s distal end to a drainage device (shown). To make it easier to connect to the drainage device, some practitioners cut the distal end of the tube. Once the chest tube and drainage device are connected, release the cross clamp that is on the chest tube. To confirm proper intrathoracic placement, look for a respiration-related swing in the fluid level of the drainage device and for respiration-related condensation levels in the tube.

Suture the tube securely to the patient’s chest with 1-0 silk or nylon sutures (shown), using a curved or straight needle.

To secure sutures, use 2 distinct through-and-through, simple, interrupted stitches on each side of the chest tube (shown). Ensure that there are no possible areas for air to leak. Each stitch should be tied tightly to the skin, then wrapped tightly around the chest tube several times to cause slight indentation, and then tied again without breaking suture. Some physicians favor locking sutures to secure a large-bore thoracostomy tube.

Place Xeroform gauze (shown) over the skin incision. Fold the gauze on itself, wrap it around the thoracostomy tube, and then push it down to the skin insertion site to create an additional barrier

Make an occlusive dressing to cover the chest tube. Turn regular 4×4 inch gauze squares into Y-shaped fenestrated gauze squares (shown), and secure them to the chest wall with 4-inch adhesive tape.

To create adequate padding, place multiple gauze sponges over the chest tube (shown) as well as between the chest tube and chest wall. To minimize how much tube movement and traction is directly transmitted to the insertion site, many practitioners create a tape “tether.”

Place tape over gauze on the chest (shown). Tape the tube along the chest wall in an “umbilicated” fashion to prevent kinking of the tube as it passes through the chest wall. This will also help to reduce wound site pain and discomfort for the patient.

Check to make sure that the chest tube is still working. Then, tape the distal end of the tube to the drainage system (shown). Be sure to tape along the long axis, so as not to obstruct your ability to see the tube and its drainage. The most common area for clots to form is at the connecting ends of the tubes

Confirm tube placement with chest x-ray (shown). Notice the final hole (arrow) is in the thoracic cavity and is seen as an interruption in the white line of the chest tube.

Confirm tube placement with chest x-ray (shown). Notice the final hole (arrow) is in the thoracic cavity and is seen as an interruption in the white line of the chest tube.

Complications of chest tube placement include horizontal placement over the diaphragm (acceptable for hemothorax; tube should be repositioned for pneumothorax), placement in subcutaneous tissue outside thoracic cavity (shown; note the subcutaneous emphysema), final hole outside of thoracic cavity, and kinked tube. Once sterility has been broken, it is never appropriate to advance the chest tube; it may only be withdrawn. Sterility is broken when the chest x-ray is performed. It is not permissible to withdraw and readvance the existing tube in a new position. If the tube needs to be repositioned by withdrawing and readvancing, then a new tube must be placed through a new incision.




0 comments:
Post a Comment